


Some quick health finds #2

Continued from

Surgery causes a big acute drop in pyruvate dehydrogenase activity through thiamine depletion (needed to use carbs fully, converting pyruvate from carbs to acetyl-coa & co2. when rats get thiamine deficient they stop eating carbs.)
https://pmc.ncbi.nlm.nih.gov/articles/PMC4472607/
takeaway: need a thiamine boost after surgery
Measurements of PDH activity and quantity and thiamine were obtained prior to surgery, at the completion of surgery, and 6 hours post-surgery. Study subjects had a mean 41.7 % (SD: 27.7) reduction in PDH activity after surgery and a mean 32.0% (SD: 31.4) reduction 6 hours after surgery (p < 0.001). Eight patients were thiamine deficient (≤ 7 nmol/L) after surgery compared to none prior to surgery
Monolaurin protects well against staph infection
https://pubmed.ncbi.nlm.nih.gov/20021093/ http://visordocs.sic.gov.co/documentos/Docs019/docs20/2014/2014006996OF/2014006996OF0000000003.PDF?713
The high amount of staph killed all 14 control mice within 1 week. but 50% survived for 30 days when given monolaurin orally.
3.2mg monolaurin given to mice weighing 15 to 20g so 160g/kg = shown effective at ~800mg-1g human dose. (higher dose might not be better).
its main effect is on gram positive bacteria like staph, instead of gram negative bacteria (gram negative bacteria e.g strep or h influenzae can be a big problem if co infected soon after a virus which is a main reason why millions of people died from the spanish flu, not the virus alone. so something else would be needed for that).
But monolaurin has antiviral activity too, effective against a broad range of human viruses (and in vivo around the same dose as shown above for staph) https://pmc.ncbi.nlm.nih.gov/articles/PMC9911909/#s3
https://onlinelibrary.wiley.com/doi/10.1111/j.1745-4565.1982.tb00429.x
Human milk contains monolaurin around 3 mg/mL. When the monolaurin is eliminated, the anti-inflammatory and antimicrobial activity is low
Its also effective at dealing with some parasites responsible for stomach bug outbreaks
BUT
it’s probably not suitable for using routinely, as its effects are skewed towards gram positive bacteria it can allow gram negative bacteria like e coli to grow. feeding ~150mg - 200mg heq for weeks created metabolic dysfunction and inflammation in mice
https://pubmed.ncbi.nlm.nih.gov/29131494/
though another study using higher dose didnt find this effect https://pmc.ncbi.nlm.nih.gov/articles/PMC6770898/ , i guess it depends on the diet / bacterial composition of the mice used.
so to be on the safer side it’s probably only suitable for short term use for a parasite or form of bacteria its known to target , like strep
Constipation - having daily routine physical movement (walking) plays a big role in bowel movements.
inactivity for 2 weeks = bowel movements went from average of 9.5 a week -> 4.5 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3748072/
Our results showed a new onset of functional constipation at the end of 35-days of bed rest in 60% of healthy volunteers as diagnosed by Rome III criteria
Feeding 0% fat high carb diet (45% -> 85% carbs) helped reverse diabetes -
lowered fasted plasma glucose and glucose peak by 10 days https://www.nejm.org/doi/full/10.1056/NEJM197103112841004
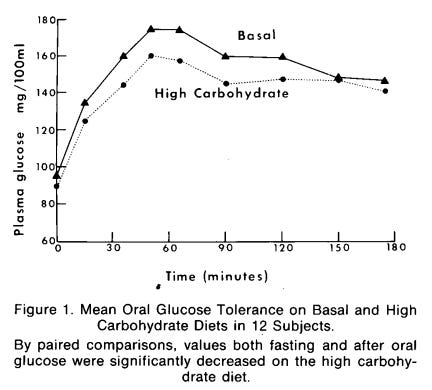
and showed lower insulin on high carb (the low 0% fat intake probably helped too as diabetes has high free fatty acids inhibiting glucose use https://diabetesjournals.org/care/article/27/9/2253/22603/Lipids-and-Glucose-in-Type-2-DiabetesWhat-is-the)
Silicon dioxide commonly added to supplements -
In this they used 100mg silica as "placebo" and "unexpectedly saw a BDNF drop in plasma". which gives support to silicon dioxide lowering neurogenesis in humans, as shown in rat studies. https://www.proquest.com/openview/50a52374cfb6b9ac6daac6d5da64492e/1?pq-origsite=gscholar&cbl=5629
Usually, addition levels of silica in soft powders can be up to 5%
a couple 500mg supplements, getting toward that 100mg,
1 study says it worsens DSS induced inflammation if the particle size is small at 10nm (even at ~15mg human dose https://www.sciencedirect.com/science/article/pii/S0006291X2032091X), but has no effect in the gut if particle size is 30nm+.
The problem is the particle size of silicon dioxide isn't regulated in supplements, so you take in a mix. If the supplement floats on water but contains silicon dioxide you can mix it and the silicon dioxide will sink to the bottom (not sure if the small particles do though).
Ray peat said it doesnt matter much what the particle is, if its small enough (e.g at the low end of the nano range) it will likely be inflammatory with barriers not being effective at keeping them out of tissues.
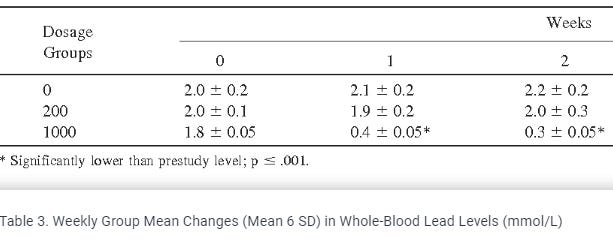
Vitamin c massively reduces blood lead levels in smokers fast,
81% blood lead decrease after 1 week on 1000mg vitamin C.
But no significant effect was found from 200mg even though blood vit C levels were similar.
https://www.semanticscholar.org/paper/The-effect-of-ascorbic-acid-supplementation-on-the-Dawson-Evans/23872e768862afea4a483c43e54669360ca5ee0f
(mechanism may be preventing re-absorption of red blood cells which contain the metals?)
If someone has a problem getting iron up in anemia or deficiency, they might need thyroid with it to stimulate absorption (instead of trying to force it up with extreme doses which gives increased toxicity)
https://academic.oup.com/jcem/article-abstract/94/1/151/2597906
(ginger might help stimulate absorption too)
Mean hemoglobin levels increased by 0.4 g/dl in the iron group [95% confidence interval (CI) 0.2–0.7, P = 0.001], whereas it increased by a mean of 1.9 g/dl in the iron/levothyroxine group (95% CI 1.5–2.3, P < 0.0001). The increase in serum iron was greater in the iron/levothyroxine group by a mean of 47.6 μg/dl (95% CI 34.5–60.6, P < 0.0001)*
15mg of iron gives the same effectiveness as high dose
"Are we giving too much iron? Low-dose iron therapy is effective in octogenarians"
https://pubmed.ncbi.nlm.nih.gov/16194646/
Two months of iron treatment significantly increased hemoglobin and ferritin concentrations similarly in all 3 groups of iron-deficiency anemia patients (for example, hemoglobin levels rose from 10.0 g/dL to 11.3 g/dL with 15 mg/d of iron therapy and from 10.2 g/dL to 11.6 g/dL with 150 mg/d). Abdominal discomfort, nausea, vomiting, changes in bowel movements, and black stools were significantly more common at higher iron doses.
Conclusions: Low-dose iron treatment is effective in elderly patients with iron-deficiency anemia. It can replace the commonly used higher doses and can significantly reduce adverse effects.
Love it! Very nutrient dense article! Thank you!